Consumption of medical services as a sociological criterion of the standard of living. Formation of market relations in health care Consumers of goods and services of health care
Economic features medical services can be summarized in three large interdependent classification groups.
first group make up the features of health services , associated with the specifics of the manifestation of the very result of the professional activity of persons employed in the area of human activity we are considering.
What are these features?
1. The result of professional activity in health care, usually, embodied in the person himself. Material services are rather an exception for health care (for example, these are x-rays, electrocardiograms, prescriptions that record the clinical diagnostic thinking of a doctor and which, when written out, begin, like books, a life independent of the will and consciousness of the author, etc.).
2.The service, as a sectoral result of healthcare, is always individual in nature. Although it itself deals with millions of people, in healthcare there is not only mass production, but also small-scale production. It is also impossible to produce (provide) health care services in advance, so to speak, for the future, and then wait for the emergence of demand and the sale of this kind of product. It is by no means the services themselves that are brought to the health care market, but only information about the services that can be provided to patients.
The consumption of a significant number of health services coincides with their production in time. The individuality of health service delivery and the creativity of many forms medical activities leads to the fact that the desired result (effect) can often be achieved only by the actions of a fairly limited circle of specialists or even by the actions of one person. Therefore, this feature of the manifestation of results in healthcare leads to the fact that the local (local) market for healthcare services is much more likely and much easier to merge with its opposite - the global market.
3. Reviewed by us result, despite all their individuality, can be varied in its physical volume. In this regard, in health care, the implementation of various options is realistic. We can imagine a doctor who deals with only one patient - the personal doctor of some celebrity. In this case, the result of his work will be individual in the literal sense. However, in order to maintain his own qualifications, this doctor, obviously, will need to have a more extensive practice.
The family nurse, based on the multifaceted nature of her functions, should achieve results adequate to the needs already in a wider physical volume, dealing with a number of individuals different ages(as a rule, starting with children of school years) and social status. Providing assistance to each member of the family, taking into account specific conditions, the family nurse can achieve the desired effect only by solving a wide range of professional tasks. She should also be competent in matters of family planning, parenting, psychology and physiology of child development, problems of overcoming stress and emotional barriers, sexual behavior, knowledge of geriatrics, etc.
4. A health outcome is complex and can be broken down into many sub-outcomes (or quasi-outcomes). This implies the importance of realizing that in order to achieve a common result - health - the efforts of both narrow specialists and general practitioners, as well as other categories of health workers, are necessary.
At the same time, it is advisable to dwell on the very concept of health as a result of medical activity.
Improving the health of the population is not only necessary, but, perhaps, the only possible a universal indicator of obtaining a certain positive result of the work of health workers in the form of a beneficial effect. Health is determined by a number of demographic and other factors. It is characterized by several main groups of indicators. The first group includes such demographic indicators as the size of the population, its composition, birth rate, mortality, natural increase, etc. The second group consists of indicators of the incidence of the population. And the third group includes indicators of the physical development of individual groups of residents. Many specific methods for assessing the result of medical activity and, accordingly, the health of the population are based on the determination of a number of indicators of a therapeutic and prophylactic nature, which are directly and more closely related to the work of medical workers.
5. Performance in health care is not directly related to the amount of costs.
6. The result is diverse in terms of manifestation and the need for repeated exposure. The range of this diversity can be quite significant: from instant results, as is the case, for example, when relieving pain, and to long-term, often painful, repetitive medical treatments that only in their totality can lead to the achievement of the goal.
7. The nature of payments for the achieved result (service rendered) can also be different. This includes direct payment, and payment through budgetary funds, and payment from funds formed in insurance organizations.
Second group definition of health service features associated with the expression of quantitative characteristics of its value . It is important to highlight a few points here:
1. The service can be provided both in the commodity (and it is in this case that it begins to have cost parameters), as well as in non-commercial form. The commodity nature of health services, and, consequently, the initial market for medical services arose already in the era of ancient civilizations (6-8 thousand years ago). With the advent of the equivalent of value, commodity relations in healthcare were transformed into commodity-money relations, which are still dominant in the industry today, although Hippocrates, the father of medicine, advised the doctor that he “behave not too inhumanely, but that drew attention not to the abundance of funds from the patient and their moderation, and sometimes he would treat for nothing, considering grateful memory above momentary glory.
2. definition the value of the cost of health care services can have several options, when choosing which the doctor inevitably faces the need to solve a complex clinical and economic problem. -
3.The cost of a health care service is not a constant value given once and for all. On the contrary, it tends to change, and more often in the direction of increase (especially with long-term treatment).
4, Maybe, despite all the uncertainty and unpredictability of the treatment and prevention process, creation of economic standards, including a number of interdependent natural, cost and relative indicators and allowing, at least roughly, to determine how much the proposed process of treatment or health protection will cost.
Third group features associated with the process of providing (production) of health services.
These features include the following features:
1. Having a large number of investors(patient, family, enterprise, employer, public organizations, including confessions, Insurance companies, state and international structures) that pay for the process of providing services. Only the joint use of various investment resources makes it possible to make the process of providing health care services continuous, high-quality and efficient.
2. Variety of business relationships which are manifested in the course of the provision of medical services and without which the activity of modern healthcare, which has undergone significant industrialization, cannot be imagined.
3. The dependence of the course of providing healthcare services on local natural and climatic conditions, which may hinder or, conversely, be favorable for the implementation of the process of treatment or prevention of various diseases.
4. The presence of an active relationship, along the line of "doctor-patient". In the process of providing health care services, all known methods of influencing the object of labor are used: mechanical, physical, chemical, biological, socio-psychological. The patient, as an object of medical influence, has the greatest activity, whichmo, on the other hand, can be directed both to harm him and to his good. In this case, in necessary cases, the conscious activity of the patient is turned off (narcosis, hypnosis).
5.Possibility of territorial movements in the process of providing health services also distinguishes the industry from many activities in the field of material production, where the process of creating wealth, as a rule, takes place geographically in one specific place.
6. In the process of providing health services, there are ability to limit effort achievement of an intermediate result with the subsequent resumption of the provision of services with a corresponding change in the conditions for the implementation of this process.
The market as an economic category characterizes the totality of economic relations arising from the sale and purchase of goods (or services). A market can also be defined as a spatial locus of supply and demand for a product (or service).
The health care market is a developed system of commodity and non-commodity exchange relations, which is an association of separate, interconnected submarkets, including:
Market of medical services;
Market of medicines, materials and hygiene products;
Market of medical equipment and tools;
The labor market of medical workers;
Market of scientific and technical developments and intellectual work;
Healthcare securities market.
The priority place in the structure of the health care market belongs to the medical services market, which can be defined, on the one hand, as a set of all medical technologies, medical equipment products, methods of organizing medical activities, pharmacological agents sold in a competitive economy, and on the other hand, as a set of existing and potential manufacturers (HCIs) and consumers of medical services (patients).
Initially arising as an instruction from the patient to the doctor, health care acquired the legal status of a service over time. Consequently, the medical services provided to patients in various institutions have also become an integral part of market relations which led to the emergence and development of the medical services market.
There are a number of classifications of medical services. All services provided in the health care system can be grouped:
By nature: medicinal; diagnostic; preventive; social; rehabilitation; medical experts; paramedical; educational; accreditation and licensing; service;
By segments of the healthcare structure: outpatient, inpatient, sanitary and hygienic, epidemiological, etc.;
By levels of medical care: pre-medical, medical, qualified, specialized;
By intensity over time: fast, urgent, planned.
Some authors propose to classify medical services also according to the qualification of the source of medical services (low, medium, high); by technology and invasiveness (routine, high-tech, invasive and non-invasive); to comply with the standard; by the time to achieve the final result; in accordance with legal regulations.
The systematized properties of medical services can be represented as:
General properties: intangibility (intangibility of character) before it is received; continuity of production and consumption of services; heterogeneity or variability of quality, inability of the service to be preserved for the future;
Economic components: cost, profitability, efficiency, service price, pricing methodology;
Medico-social properties: timeliness, accessibility, quality.
Let us dwell on a few general and basic characteristics of medical services that are important for the healthcare market.
Intangibility is the inability to see, taste, hear or smell a service until it is purchased. For example, a woman who comes to a plastic surgeon will not see the result until she buys his service, i.e. agree to the operation. The patient who came to the doctor cannot know in advance the result of his visit. The buyer (patient) is forced to take the seller's (doctor's) word for it. This is a key moment in the economics of health care and analysis of the production and consumption of health services. To expand the possibilities of studying the properties of medical services before receiving them, the following measures are proposed:
Increase the tangibility of the service (provide photographs or drawings of any analogues before the service is provided);
Emphasize the patient's attention to the benefits of the medical service;
Assign a brand name to a medical service for sale on the market;
Involve any competent person in the promotion of your service.
inseparable from the source. The service will not be the same if instead of the expected specialist doctor known to patients, the treatment session is performed by another doctor. The doctor and his service are inseparable. You can overcome this limitation in the following way:
A service provider (physician) may learn to work with multiple audiences (eg, a psychotherapist forms a group);
The service provider (physician) can learn to work faster (increase service intensity);
Prepare a lot of service providers - doctors in health facilities.
Quality inconsistency. The quality of services varies widely depending on the various characteristics of providers (physicians), as well as the time and place of delivery. For example, an experienced surgeon operates much better than a freshly graduated surgeon. However, the same doctor treats differently depending on his physical condition, the availability of medicines and equipment. To reduce the “volatility” of services and ensure quality control, you can:
Develop quality standards for medical care;
Allocate funds to attract and train really good specialists (medical training);
Constantly monitor the degree of patient satisfaction through surveys, questionnaires, followed by the formation of a system marketing information about the quality of medical care.
Inseparability of production and consumption of services. The service cannot be produced for the future and saved. In this regard, many doctors in Western Europe also charge a fee for non-attendance patients, since the value of the service exists even at the time of the patient's non-appearance. The inability of a medical service to be stored requires the development of a strategy that ensures a tighter alignment between patient demand and facility supply, for example:
Establishment of discounts and other incentives, in particular to shift part of the demand from the peak period to the period of decline in demand;
Introduction of a system of pre-orders for medical services (doctor's appointments);
To serve an additional flow of patients during the peak period, train staff to combine functions, hire temporary employees.
According to G.K. Maksimova et al. (1996), the production and consumption of health services is a holistic process. concept life cycle medical service includes the following stages of its implementation:
Examination and diagnosis of the patient's condition;
Designing the provision of a medical service: understanding the task (final result), making a decision to provide a service, planning (choosing) a technology for providing a service;
Provision of medical services;
Consumption (use) of a medical service;
Self-destruction of the service or the resumption of a repeated need for it.
Market relations express a certain economic isolation of producers and consumers of products and services. The market mechanism is the process by which sellers and buyers interact to determine the price and quantity of goods produced, whereby demand, supply and price are its main elements.
The mechanism of the medical services market also functions due to the interaction of three main components: demand, supply and price.
Demand is the quantity of medical services that patients are willing and able to purchase over a certain period and at a certain price.
The offer is the number of medical services that can be provided in a certain period of time in a given territory by a given medical institution (doctor).
Price - monetary value the value of the product (or service).
When demand and supply interact, all other things being equal, an equilibrium market price is formed, the point of intersection of the supply and demand curve, it is the equilibrium price that mutually suits both the seller and the buyer (Fig. 4).
T is the equilibrium point, P" is the equilibrium price, Q" is the equilibrium quantity of medical services at the price P", which will be purchased by patients at a given point in time and will be provided by doctors in the same period
The key concept expressing the essence of market relations is the concept of competition. In general, competition can be defined as a type of relationship between producers regarding the setting of prices and volumes of supply of goods and services, as well as between consumers regarding the formation of prices and the volume of demand in the market. From the standpoint of the structural organization of the market, the number of producers (doctors, healthcare facilities) and the number of consumers (patients) participating in the exchange process are of decisive importance.
Depending on the ratio between the number of producers and the number of consumers, the following types of competitive market structures are distinguished: perfect competition market, oligopoly, monopoly, monopsony, monopolistic competition. Each of the structures has its own characteristics of price formation, supply and demand, in addition, in the health care market, as indicated, special properties of a medical service are added.
Thus, the market of perfect competition presupposes the presence of a large number of independent producers of some homogeneous product, on the one hand, and a mass of isolated consumers of this product, on the other. The structure of communication is such that each consumer, in principle, can purchase a product (or services) from any manufacturer, in accordance with his own assessment of the usefulness of the product and its price. Each producer can sell the goods to any consumer, according to his own benefit. None of the consumers acquires any significant part of the total supply and none of the producers can satisfy any significant share of the total demand. The market of perfect competition is the most efficient structure that allows the best allocation of resources.
If there are any objective restrictions for sellers and buyers, then there are structures of imperfect competition that require adjustment by the state.
Analyzing from these positions the healthcare sector in many developed countries, it should be noted the presence of state restrictions, acting in a variety of forms.
For example, the American Medical Association, which unites about half of all private practitioners, plays an important role in artificially curbing the supply of medical services in the United States. It limits enrollment in medical faculties, increases tuition fees, controls the influx of migrant doctors and their access to medical practice. It should be noted that there are additional artificial barriers for medical service providers when they enter the market: frequent attestations, the need to obtain a new license when a doctor moves from state to state, etc.
The limitations of competition and information noted above mean that the market for medical services differs significantly from the market for perfect competition. Under perfect competition, if a firm discovers a better way to produce a product, it simply lowers prices and thus steals buyers from other producers. Production is always efficient, and prices reflect the production costs of the most skilled producers. If these conditions are not met, then those producers can survive, whose prices significantly exceed the cost of production. When the product is heterogeneous and the buyer is not too well informed, then it is difficult for him to determine what more low price- a signal about the possibility of a more profitable purchase or about the low quality of the product / service. And when buyers are informed about prices, then firms can raise them above the equilibrium price level only with a limited number of sellers or a limited number of buyers.
It is possible to schematically show the differences between the product market of perfect competition and the market structure that is typical for the medical services market as a whole (Table 4).
Table 4

Based on the above comparison, it follows that the market for medical services, in terms of organizational structure, is an imperfectly competitive market. At the same time, in terms of its main characteristics, it is closer to structures that are classified in economic theory as a market of monopolistic competition and a monopoly. These circumstances inevitably leave their mark on the behavior of health care providers (HCPs), changes in their primary goals, the pricing system, which also requires regulation of the ongoing processes in these market structures from the side of the state.
Health care, as a branch of the public economy, has a number of characteristics that violate the market mechanism:
Some medical services have the property of "public goods" (or "public goods") (one of the features of "public goods" is their ability to extend their consumer effect to persons not participating in the market transaction);
Lack of awareness of the consumer, information "asymmetry" of the producer and consumer of medical services deforms the usual interaction of supply and demand;
The special role of the principle of equality in obtaining medical care: the volume and quality of consumption of medical services cannot be determined only by the level of solvency of the population - this, of course, violates the mechanism of market pricing in healthcare.
In this regard, it is extremely important to pay attention to the factors that determine the demand and supply of medical services. The key role here is played by the price of a medical service, which, on the one hand, determines supply and demand, and on the other hand, under conditions of its free change, balances them. In order to build forecasts of the relative change in the magnitude of demand or supply when the price changes, it is necessary to know the quantitative parameters of these changes. The most common quantitative characteristic of demand is the so-called price elasticity of demand.
Price elasticity of demand is measured as the ratio of the percentage increase in the volume of demand for a product (service) to the percentage decrease in the price of this product, all other things being equal. It shows by what percentage the quantity demanded will increase if the price of the service decreases by one percent. Demand for most medical services has a low elasticity, which means that the elasticity coefficient is less than one. According to a number of US experts, the price elasticity of demand for inpatient medical care averages 0.7 (with the exception of cosmetic surgery), and in many cases it ranges from 0.2 to 0.7. This means that when the price of medical services rises, demand decreases to a lesser extent than the price rises (if the price rises, say, by 10%, demand will decrease by 2-7%).
Supply and demand are affected not only by price, but also by a number of other factors: the determinants of supply and demand. The determinants of demand include the level of income and solvency of the population, the structure of medical services and their cost, the prevalence of diseases, and the level of awareness of patients about them, “forcing demand” by medical workers, and much more. Determinants of supply are such factors as the number of doctors, the cost of medical equipment, the improvement of medical equipment, the emergence of new competitors, etc.
MINISTRY OF HEALTH AND SOCIAL DEVELOPMENT OF THE RUSSIAN FEDERATION
NORTHERN STATE MEDICAL UNIVERSITY
INSTITUTE OF PUBLIC HEALTH, HEALTH AND SOCIAL WORK
Test
in the discipline "Health Economics"
Topic: The health care economy in the market system of economic relations.
Health care market.
Completed:
Checked:
Arkhangelsk
Introduction
Economic relations in health care, namely, the relations of production (creation), distribution, exchange and consumption of medical goods, have an indirect impact not only on the life and health of a particular person, but also on the state and reproduction of such a social resource and the potential of society that contributes to the development and prosperity of the nation as public health.
Public health is a medical and social resource and the potential of society that contributes to national security and ensures the quality of life, due to the state of health of the population. The most important condition for the reproduction of this social resource is the implementation of a coordinated state policy, carried out simultaneously by various branches of the national economy and sectors of the economy in the field of economic growth and social well-being, where health care plays a significant role. Therefore, public health depends on the quality of economic relations both within the health care system and outside it, on their orientation towards improving the health of the population. All this necessitates the search and justification of ways to solve an important national economic problem - the development of economic relations in health care, focused on improving the health of the population.
Healthcare occupies an exceptional place in a socially oriented economy, it is here that socially consumed goods are produced - medical services. Recently, health care has been increasingly involved in the economic turnover of society, which is facilitated by the active functioning of medical institutions on a market basis.
1. Market economy and its essence
A market economy is an economic system in which the market plays the role of the main regulator of economic relations. In this system, the distribution of resources and the formation of proportions that satisfy social needs are carried out with the help of market mechanisms through the movement of supply and demand, through a system of prices and profits.
The main feature of a market-type economy is emancipation from external interference, submission to the laws and will of people, forms and methods economic activity giving the opportunity to fully manifest economic independence. The market economy is the economy of unenslaved, but civilized entrepreneurship. It cannot be considered unambiguous, characterized by a single property. In accordance with its purpose, it appears that this is a large market economy. But that's not the point market economy. The economy is not only a market for buying and selling. Rather, we should talk about the economy of market relations that permeate the reproductive process, including production, distribution, exchange, consumption of a social product.
There is no single principle for the construction and functioning of a market economy, i.e. the principle of "market". Actually we are talking about the whole system, a set of principles that, taken together, taking into account their interconnection and interaction, characterize the market economy, the mechanism of its action. The market economy is a complex system economic ties and relations, which requires an analysis of supply and demand, production costs, money economy, economic growth, etc.
The fundamental characteristic of the market system is private property, which allows individuals or enterprises to acquire, control, use and sell material resources at their own discretion. On the basis of private property, freedom of enterprise and freedom of choice are realized.
Free enterprise means that a private enterprise has the right to acquire economic resources, organize the process of production from these resources of goods and services of its own choice and sell them on the markets, based on the interests of the company. An enterprise is free to enter or leave any particular industry.
Freedom of choice implies that the owners of material resources and money capital can use or sell these resources at their own discretion. It also means that workers have the right to do any kind of work for which they are capable. Finally, it allows consumers to freely, within the limits of their monetary income, buy goods and services in such a set that they consider most suitable for themselves. The freedom of consumer choice is the broadest of these freedoms. The consumer in a market economy occupies a special position; in a certain sense it has sovereignty. The freedom of entrepreneurial activity ultimately depends on consumer preferences.
Freedom of choice is based on self-interest. Each economic unit is able to do what is beneficial to itself. Entrepreneurs strive to get more profit, owners of material resources - a higher price when selling or leasing these resources, workers - more pay for their work, consumers of products or services - to purchase this benefit at the lowest price.
Freedom of choice is the basis of competition, or economic competition. Competition provides:
- the presence on the market of a large number of independent buyers and sellers of each good (no buyer or seller can present a demand or offer for such a quantity of products that could affect its price);
- there are no artificial legal or institutional obstacles to the expansion or contraction of individual industries (a manufacturer can easily enter or leave an industry).
At the same time, in the total mass of principles and features of a market economy, there is no equivalence, understood as the relative equality of the significance of each of them. It is possible to identify the leading main principles that are of decisive, decisive importance. Other principles turn out to be particular, derivative, secondary.
Any economy develops on the basis of objective laws, they are the same for any socio-political and socio-economic system, they are universal, general in nature, and in this respect are similar to physical and biological laws. But the laws of economics manifest themselves in the activities of society and individuals, operate in a certain socio-economic environment. And this environment is not passive. Its main elements - a person, social groups, society, power - within the conditions and restrictions determined by objective laws, have a significant degree of freedom of choice, act in accordance with their own will.
Thus, there is always a space of economic actions, the content and method of implementation of which depend on people and are determined by them either individually, or in a group, or in a public way. The meaning of a market economy is that it forms a fairly free, liberated space for economic activities carried out within the framework of laws, rules, and norms of economic behavior established by the state and society.
For example, the laws of supply and demand underlying the market pricing mechanism do not unambiguously determine the value of prices. Specific values of prices and even methods of pricing are determined by the rules of behavior of participants in the economic system. The most important rules of this kind, observed by the majority of participants, form the principles. The more fully the principles are consistent with the laws, the more efficiently the economic system operates, the more fair and objective it is.
Unlike economic laws, principles do not have a universal universal character, they depend on the type, type of socio-political, economic system, and in a certain sense even characterize the system from the point of view of the dominant state ideology and social, social psychology.
Considering, assimilating the principles of a market economy, its differences from a centrally controlled, state-owned economy, it is necessary to understand that neither one nor the other economy exists in its pure form. A market economy is essentially a mixed economy in which the market is combined with state regulation.
The mechanism that coordinates the activities of all subjects is the market and prices. The market is a mechanism by which contact is made between the carriers of supply and demand. Based on the coordination of the interests of these two subjects, a system of prices for products and services is formed.
2. Market relations in healthcare
Traditionally, it is believed that a full-fledged market cannot be formed in the field of healthcare. The simplest market relations, which are so understandable in other sectors of the economy, do not work here due to the failure of the market, since healthcare, as a branch of the public economy, has a number of characteristics that violate the operation of market mechanisms.
It is believed that, firstly, in healthcare, the level and volume of consumption of required medical services cannot be determined only by the level of a person's ability to pay. This applies, first of all, to emergency medical care, which is provided free of charge in many countries of the world, even to people who do not have funds and insurance. Moreover, it has been proven Feedback between the level of personal income (i.e. real solvency) and the need for medical care. Thus, in the UK, out of the total number of cases of diseases, 37% occur in the 10% of the poorest families, who consume almost 50% of all health care resources. Security equal opportunity in the consumption of medical services dictates the need to redistribute the health budget (which is realistic only under state regulation) in favor of those most in need - children, the elderly, chronically ill people, people with low incomes, based on the principle of social solidarity: the rich pay for the poor, the healthy - for the sick, the young - for the old. However, this actually destroys the principles of market pricing, since the costs of treatment are transferred to the solvent population.
Secondly, it is commonly believed (and this is true to some extent) that the consumer of medical services cannot judge the level and quality of the required medical care (due to the lack of special knowledge, physical and mental condition). Unlike other markets, in healthcare, it is not the consumer (patient), but the manufacturer (medical worker) who determines the volume and level of medical services provided. Doctors simultaneously act in several faces: producers of medical services, agents of patients who determine the measure of their needs, the volume (and sometimes cost), the quality of treatment and the medical services they provide. As a result, there is a conflict between the medical and economic interests of doctors and patients. In addition, the patient, as a rule, does not have objective information about when, what kind and to what extent he will need medical care. This significantly hinders the purchasing initiative of the population regarding the purchase of health insurance or participation in health and preventive measures. This asymmetry of interests of medical workers and patients (producers and consumers of medical services) deforms the usual interaction of supply and demand and, in turn, determines the specifics of market mechanisms in healthcare.
Thirdly, a part of medical services (sanitary and hygienic, anti-epidemic, preventive, etc.) has the properties of public goods, i.e., unlike goods for individual consumption, is an object of collective consumption, most often non-targeted. This includes preventive, sanitary and epidemic measures, vaccination, which are immediately provided to a large number of people, and the positive effect extends to the entire population as a whole.
3. The health care economy in the market system of economic relations
An analysis of the external conditions for the functioning of healthcare in a market system of economic relations shows that today the development of the social sector of the economy requires access to data on the closeness of the relationship between the health of the population and the levels of material support and education, the nature of hygienic behavior and the state of the environment.
In the changed conditions, the development and use of optimal methods of payment for medical services requires taking into account the theoretical provisions of neoclassical economic theory, which considers medical services as a purely "economic commodity" .
The main characteristic of the modern market economy is a pronounced social orientation. Its essence lies in the subordination of all economic activity the interests of the development of society by creating conditions for the most complete disclosure of the inner potential of the personality of its constituent individuals. As historical experience has shown, the developed countries of the world were able to solve the tasks assigned to them to humanize national models of a market economic system. The transition of the Russian economy to market principles of management has necessitated systemic transformations in society, covering almost all spheres of people's life. The main task of the present period of social development was the creation of a socially oriented economy. The need for its formation is associated with the action of a number of objective factors that reflect the requirements of the current stage of development of civil society:
Satisfaction of basic needs and provision of normal living conditions for all members of society without exception;
Creation of conditions for free creative labor, the main driving force of scientific and technological progress and economic growth;
Harmonization of social relations between individuals and social groups.
The urgent need to develop a socially oriented economy is due to the impact on the health and well-being of the population of many factors that go far beyond the competence of the health sector. Health services are only to a limited extent able to influence the main causes of morbidity in a country. The state of health of the population is largely determined by the interaction of other interrelated factors: socioeconomic status, behavior and lifestyle, genetic predisposition and the state of the environment. They are closely related to the state of the national economy, the humanization of which is an indispensable condition for eliminating the factors of deterioration in the health of the population and ensuring the economic development of the country.
The creation of a socially oriented economy in our country requires the combined use of the principles of the socialist social system with market incentives. The social orientation of the Russian economy should be aimed at achieving several goals. Firstly, it is ensuring a rational level of consumption for the majority of the population by saturating the market with consumer goods and services while reducing the differentiation in the level of consumption of goods to the extent that incentives for skilled labor and effective entrepreneurship remain; secondly, the creation of conditions for skilled creative labor with a qualitative change in the structure of the economy: reducing the share of heavy physical labor to a minimum, environmentally hazardous industries and development of industries focused on the consumer market; thirdly, the creation of an effective system social protection population.
The main condition for effective socialization of the economy is the development of the social sector. It unites sectors of the national economy, whose activities are aimed at meeting the social needs of society. This sector forms the sphere of non-material production, i.e. service production (tertiary sector). In it, just as in the primary (mining industries) and secondary (manufacturing industries) sectors of the economy, material, labor and financial resources are used, investment activities are carried out. Branches of the social sector produce predominantly intangible goods (services). This is a special type of economic benefits provided in the form of professional activity that do not have a material expression and exist only at the time of their provision.
Economists refer to services as a special kind of economic goods. According to the definition of the classic marketing theory F. Kotler, a service is any event or benefit that one party can offer to another, and which is basically intangible and does not lead to taking possession of anything. A professional service is a transaction, the actual completion of which is embodied by the invested work of a professional. One of the varieties professional services are medical services. A medical service is a structured unit of medical care; This is an event or a set of measures aimed at the prevention, diagnosis and treatment of diseases that have an independent complete value and a certain cost. The human body as an object of medical activity and the targeted professional impact on the state of his health as a subject significantly distinguish the medical service from the world of ordinary goods and other professional services. When developing organizational models for the provision of medical care, it is important to take into account the characteristics inherent in all types of services;
The intangibility of the service, due to the frequent absence of well-defined guarantees, increases purchasing risk, which is much more difficult to assess than in transactions for the sale of ordinary goods. The intangibility of the service requires advanced consumer confidence and is compensated by the material conditions of its provision. Licensing is used to overcome this feature of services;
Source inseparability is that the service does not exist before it is provided. This makes it impossible to pre-evaluate it in each specific case. It is only possible to compare expected and received benefits. Accreditation and certification serve as a way to compensate for this property of services;
Variability of quality (uncertainty, variability). In connection with the possibility of an individual reaction of the body, the uncertainty of the final result increases, which may be complete, incomplete or absent altogether. Overcoming this property is achieved by using standardization and unification;
The non-conservation (non-accumulation) of the service necessitates its advance payment.
The use of the market concept in healthcare is based on the recognition of medical services as an economic commodity that can be bought and sold on open market. Economists group all known economic goods into four large groups: general, public, collective and private goods. The main classification criteria for grouping economic goods are their exclusivity and competitiveness in the process of consumption.
Many health care services are considered by supporters of neoclassical theory as purely private (individual) goods. They consist of small enough units and can be purchased by individual buyers. As a result of such a purchase, the product is used by the one who bought it, or, in other words, the process of consuming private goods is subject to the rule of "exclusion". From this point of view, the health benefits of consuming these products are only received by the person using them (for example, buying aspirin to treat a headache). For this type of product, according to the standard neoclassical model, the way to choose to finance them is through pricing based on marginal cost. From an economic point of view, in practice it turns out to be an optimal investment.
Some health care services are purely public goods, since their benefits are used by all members of society without exception. They consist of large units and cannot be sold to the individual consumer. The process of their consumption is not subject to the "exclusion" rule. The public can enjoy the benefits of public goods without incurring the costs of acquiring them. Examples of public goods are some environmental health interventions (air quality control and water pollution abatement). Charging the user for these services seems unrealistic, since non-payers will enjoy the same benefits as payers. Thus, there are no incentives to pay for such services (the so-called "traffic hare" or "free rider" problem). Since these goods are difficult to express in prices and sell to the individual consumer, it is also difficult to find a manufacturer who, on his own initiative, will produce and offer them. At the same time, there is a public need for such goods, so the state takes upon itself the provision of the production of goods and services for public use and organizes their forced purchase through the system mandatory payments(taxes).
Finally, many health services are viewed by economists as mixed goods: individuals benefit from the use of services, but others, although not directly involved in the transaction between producer and consumer of services, also benefit. An example is the treatment of infectious diseases such as tuberculosis or syphilis. It protects not only the sick, but also those whom these patients would infect if the treatment had not been carried out. In this case, social benefits exceed private benefits. Therefore, the use of pricing based on marginal cost leads to a decrease in the volume of service use in relation to the socially optimal volume. For these goods, economists consider it appropriate to introduce subsidies in order to raise the level of private demand to a level that equalizes social benefits with social costs and thereby maximizes the expected welfare of society. The economic consequences of introducing cost sharing in this case can be heterogeneous. Subsidization involves payments by consumers of services of varying amounts, ranging from zero to a significant percentage of marginal costs. In conditions when the price of a service is lower than the marginal cost, prerequisites are created for an increased volume of consumption of medical services. When describing the reason for their excessive consumption, analysts use the concept of "moral temptation".
In the conditions of a market economic system, payment for medical services can be carried out in different ways. Depending on what type of economic goods these or those medical services belong to, one of three alternative payment options is used: individual, collective or public method of financing medical care.
You can pay for medical services on the spot ( individual way payment). Such a system is called a fee system and is convenient only for the wealthy part of the population. Since the decision to purchase individual goods is made by an individual independently, the volume of their production is determined by the need and solvency of buyers.
The majority, having lost their source of income in case of illness, are not able to pay for the necessary medical services and medicines. Therefore, already in the XVIII-XIX centuries. Buyers of medical services, in order to ward off the rule of "exclusion", began to unite in mutual aid societies, create sickness funds and various funds, i.e. insurance organizations. So, when buying goods for individual use, a collective method of financing medical services was developed, a system of social insurance arose.
The content of the initial stage of the development of social insurance as a form of social mutual assistance was the consolidation of small insurance contributions of the population for general use, with the obligatory condition of refusing to return them. Its basis was the principle of social solidarity: the rich pay for the poor, the young for the old, the healthy for the sick. At the same time, the activities of insurance organizations contributed to the solution of two important social problems: increasing the solvency of customers and ensuring the availability of medical care to low-income groups of the population. Market regulators remain active in the insurance system. Even in the case of a high degree of socialization and state regulation, the consumption of medical services is individual in nature, which is ensured by keeping personal records of the total cost of medical services received by each citizen during the year. Personal accounting is the basis of the financial activity of an insurance organization; without it, there can be no insurance.
Further development of the insurance system is associated with the growing importance of social mechanisms in health insurance. Over time, trade unions and other social movements and organizations have achieved from the parliaments the adoption of laws on compulsory health insurance for employees and the participation of employers in paying health insurance premiums. For the first time in the world, the compulsory health insurance system was introduced in Germany. Its basis was the code of laws adopted by the government of Chancellor Otto von Bismarck in 1883, 1884 and 1889. Only the minimum volume of medical services was supposed to be provided at the expense of insurance funds. At the same time, additional, mostly private and profitable insurance developed, which provided medical services that went beyond the mandatory programs.
The subsequent transformation of the financial health care system in the 20th century is associated with the use of new political and ideological strategies in the field of public health and the development of population medicine, the object of which was not an individual patient, but large groups of people. During this period, in many countries of the world, health care switched to budget financing, i.e. the public method of paying for medical services began to be used, the so-called budgetary or "free" medicine arose. As a result, the majority of the population began to consider health care as an indivisible social product. Since the process of consuming a public good is not subject to the rule of "exclusion" and everyone has the same access to it, people have the impression that the public good is free, and as a result, unreasonable excessive consumption of it has arisen. Under conditions of compulsory payment for public goods, the decision on the volume of their production is made at the state level. Those who decide on the required volumes of production of a public good, consider the increased scale of consumption as evidence of a growing need for it and expand production. Thus, a vicious circle arises that generates overconsumption and overspending of resources in the budgetary health care system, or "free" medicine.
Thus, the peculiarities of medical services as an economic commodity cause serious difficulties in choosing the optimal model for organizing and financing the healthcare system. There is no doubt that it should be of a mixed nature and have several sources of funding that are independent of each other. At the same time, the part of the system that is inherent in individual consumption should be managed by market regulators, and the social injustice resulting from the implementation of the "exclusion" principle should be mitigated through the operation of insurance mechanisms. The same part of the system that is in the nature of public consumption must be subject to political decisions. In practice, the implementation of this regularity is complex and very ambiguous. However, its complete oblivion entails serious consequences. In particular, one should be aware of the different impact of charging patients on the amount of medical services they consume. This effect is explained by the fact that prices often prevent the use of medical services when their payment is a large share of the family budget. As a result of reduced consumption of medical services and delays in examination and treatment, people's health may deteriorate to the extent that an increase in the availability and quality of medical care could favorably affect the health of individuals, social groups and society as a whole.
4. The health care market
A health care market occurs when there is a potential for exchange. The health care market is determined by the presence of two parties - those who need medical services and those who offer them; the presence of market entities - the necessary medical institutions where the sale and consumption of a medical service or product can be carried out; the presence of freedom to choose mutual offers of producers and consumers of medical services.
Along with the medical services market described above, the concept of a market in healthcare includes a whole system of separate elements, interrelated markets: the drug market, the labor market of medical personnel, the market for scientific medical developments, the market for medical equipment and technology, the securities market (the last element takes place only with a developed market).
The market in general, including in healthcare, performs a number of essential functions:
1. Information. Through changing prices, the market provides production participants with objective information about the socially necessary quantity and quality of services and other products supplied to the market.
2. Intermediary. Economically isolated producers should share the results of their activities. Without a market it is not possible to determine the mutual benefit of their activities.
3. Pricing. The market receives services of the same purpose, but differing in costs. The market recognizes only those costs that meet the conditions for the provision of the bulk of services of this type, it is them that the consumer agrees to pay.
4. Regulatory. Through competition, the market regulates the reduction of costs per unit of services provided, the improvement of their quality, and encourages the scientific and technical process.
Speaking about the development of market relations in healthcare, one cannot absolutize the significance of this process. Health care as a specific area affecting the vital important questions will obviously not be able to fully and completely focus only on market relations (at least for now). Socially significant types of medical care will remain, which should be subsidized by the state - the fight against AIDS, tuberculosis, epidemics, infectious diseases, etc.
In order for the pursuit of profit, for profitable types of medical services, not to have a detrimental effect on the entire healthcare system, an effective economic mechanism must be developed that combines budget financing, financing from local budgets, the use of insurance premiums and the transfer of certain types of medical care to a paid basis.
The solution of these issues is associated both with a general improvement in the economic situation in the country, and with a change in the economic mechanism of healthcare itself.
In health care systems built on the Soviet model, the volume and level of medical care, with all the declaration of equality and social justice, had a high degree of privilege. A special system of medical care was created for the leadership of the party and the country. With limited resources available for health care, some priority was given to workers and children. Even today, all this does not prevent us from asserting that the availability of qualified medical care was provided by the state, regardless of the patient's social status, place of residence, etc.
The fundamental essence of the modern period of reforming the domestic health care system, along with others, is characterized by objective conditions under which a medical service becomes a commodity, and the relationship between producers and consumers of medical services (in particular, a doctor and a patient) essentially begins to be defined as marketing with a predominant role of the patient. Such manifestations of the relationship between a doctor and a patient characterize the system of compulsory medical insurance, the introduction of which in Russia has been carried out since 1991.
Classical civilized market relations, as you know, are subject to economic laws, are specific in management and are in conflict with the methods of administration. In the field of market relations, medical care, as a kind of production activity, is filled with economic characteristics.
Prior to that, conditional groups of patients (patients with one disease, decreed contingents, persons in dispensary observation groups, etc.) begin to correlate with structures characteristic of the market. The field for the implementation of relationships in medicine are certain segments of the medical services market, the diversity of which in form and content reflects in health care both in social structure society is one of the principles of democracy. One of the characteristics of the medical services market in liberal healthcare systems is its segmentation, i.e. targeting the sale of medical services to certain consumer groups.
The latter fact is reliably confirmed by separate studies of domestic authors, according to which the following layers are conditionally distinguished in modern Russian society (data taken from the book “Fundamental Foundations of Health Policy”, edited by O.P. Shchepin, M., 1999):
Oligarchy and governing bureaucracy - up to 7%;
Middle class - up to 12%;
The layer of conditional poor - more than 60%;
The lowest groups of the population - less than 12%;
Desocialized citizens - up to 9%.
The interaction of all subjects of the healthcare system, especially in the system of compulsory health insurance, the definition of their functions, and, consequently, the formation of types and forms of relations between a doctor and a patient, is naturally associated with the specific characteristics of the population as a consumer of medical services. And such characteristics, as noted by A.V. Reshetnikov (2000) are gender, age, marital status, occupation, level of education and income of certain social groups, as well as psychographic data: belonging to a particular social stratum, lifestyle, personal and behavioral qualities.
It is on the basis of the real stratification of society that it is necessary to determine approaches to the specificity of the medical services market, its segmentation, especially in matters of characterizing industrial relations in these segments.
Objectively, in the activities of medical institutions, there was a process of classifying patients into groups with different needs and requirements, characteristics or behavior. It is these criteria, along with some others, that determine segmentation of the medical services market in marketing systems, i.e. the specification of medical technologies and medical procedures that satisfy a certain demand of a patient (client) is objectively and naturally focused on specific potential consumers of a certain market segment. And all this, in turn, determines, in particular, the economic specificity of the doctor-patient relationship.
Given the above classification of the stratification of society (or, in principle, relying on any other possible classification), it is methodologically justified to single out segments of the medical services market that meet these conditional criteria.
In the study of this problem, in search of solutions to the outlined contradiction between the needs for medical services and the satisfaction of demand, the use of the medical services marketing model, a fragment of which is shown in Fig. 1, helps.

Fig.1. Model of the medical services market.
When studying the relationship between the elements of the model, an attempt was made to clarify the criteria for distinguishing the essence of medical care and medical services, as well as to outline the essence of a medical procedure in the corresponding market segment. In any of the segments of the medical services market, the medical needs and needs for medical care of a patient (client), regardless of belonging to a particular social stratum, are not related to his personal or social well-being: pathological conditions (illness) and the need to be healthy are specific categories, more biological than social. In this sense, regardless of the social status of the patient (client), a specific type of medical service that meets a certain standard is interpreted by a specific psychosomatic state and the purpose of the treatment. At the same time, the demand and the possibility of acquiring a specific medical procedure from a variety of procedures that are adequate for a certain type of medical service are directly related to the patient's well-being and ability to pay.
Thus, health care systems based on objective economic laws with many determinants are characterized by certain market segments. Segmentation of the medical services market makes it possible to provide medical care (to satisfy a specific demand) both taking into account the individuality of the patient and taking into account the mass consumption of medical services.
Conclusion
Healthcare has its own characteristics, suggesting the primacy of medical results over financial ones. And in this sense, the scope of market relations in health care is somewhat limited. We are talking about the need to clearly distinguish between areas where the achievement of the best medical indicators is possible on an economic basis, and areas where this must be achieved by administrative, public and other measures.
In order to economic relations in health care were purely market-based, a match must be achieved between the entity paying for medical services and the consumer of these services. In other words, in purely market relations, everyone must pay out of his own pocket for the service rendered to him. However, in the health care system there are a large number of publicly consumed services (primarily a set of preventive measures and the activities of sanitary and epidemiological surveillance institutions), which cannot and should not be paid for and consumed by anyone individually.
The healthcare organization should be based on complementary and balancing contributions of three parties: the state, healthcare organizations and the population, as well as principles that stimulate, on the one hand, the rational consumption of medical services and the population's concern for their own health, on the other hand, the motivated desire of healthcare organizations to provide quality medical care to the population, improve the quality of life of patients.
Literature:
1. Grigoriev Yu.M., Istomina L.B. // Economics of health care. - 1999. - N 2. - S. 10–14.
2. Komarov Yu.M., Ermakov S.P., Ivanova A.E. etc. // Healthcare Economics. - 2000. - N 7. - S. 5–12.
3. Svetlichnaya T.G. Health care in the market system of economic relations // Glavvrach, 2008, N 8.
4. Taranov A.M. // Economics of health care. - 1998. - N 2. - S. 12–14.
5. Shamshurina N.G. Economics of a medical institution. - M.: MTsFER, 2001. - 278 p.
6. Sharabchiev Yu.T. Market relations in healthcare and possible mechanisms for their implementation in the conditions of state regulation // Medical News - 2006. - No. 3. - S. 83-88.
7. Sheiman I.M. Health care management and financing reform. - M., 1998.
8. Shishkin S.V. // Economics of health care. - 2000. - N 8. - S. 10-15.
9. Shchepin O.P. // Prob. social hygiene, public health organization and the history of medicine. - 1999. - N 3. - S. 7-10.
10. Shchepin O.P., Gabueva L.A. Organization and economics of entrepreneurial activity in health care. M., MTsFER, 2006.
The healthcare market is part of the general economic market environment. It has the same characteristics, but it has its own specific features.
Part of medical services has the character of "public goods". Their consumer effect extends to the whole of society and even to persons not participating in the market transaction, for insolvency or for other reasons. Everyone benefits from these services.
Public goods include sanitary and anti-epidemic, preventive, medical measures, the result of which is the prevention of diseases and the improvement of the health of the entire community.
Meeting the needs of the population in these services is carried out by sanitary and epidemiological stations, health centers, which are financed from the budget.
"Asymmetry" of information in the medical services market affects the economic relations between the provider of medical services and their consumer.
On the one hand, the insufficiently informed patient about the state of his health, the volume and price of medical services allows the doctor to influence the demand (“demand imposed by supply”) and realize his economic interests (offer medical services that are not mandatory to achieve a clinical result). Therefore, there is an increase in prices in the hospital sector by 60% (USA).
On the other hand, the patient may have a "moral temptation", without any obvious need, for expensive diagnostic tests, surgical interventions, medicines, and with health insurance - frequent visits to the doctor. This is due to the fact that the patient is not aware of the price of medical services, which leads to financial and moral costs.
Accessibility and equity in health services is the main strategy of modern health systems. It is based on the historically established principle of social solidarity: the healthy pays for the sick, the rich pays for the poor; the one who works pays for the one who does not work. The principle is introduced with the participation of the state (compulsory health insurance).
In the world, the volume of medical care consumption is not determined solely by the patient's ability to pay, but in some cases depends on the urgency of medical care. Even under conditions private system health care, emergency medical care can be provided free of charge.
Producers of medical services also act as their sellers. This is due to the combination in space and time of production, sale and consumption of medical services.
Complex structure of demand for health services associated with the need for their personification and individualization.
Peculiarities of the dynamics of demand for medical services characterized by her hesitation depending on the season of the year (it decreases in summer, and in autumn-winter period increases), on the structure of the population in various territorial segments of the healthcare market.
The result of medical activity can be determined only after the consumption of the service, it is difficult to express it in terms of value.
High variability market conditions associated with changes in the epidemic and environmental situation in the country.
Feature of territorial segmentation market depends on the structure of the incidence of the population of the region.
Limited access to the medical services market due to the presence of special higher medical education, testing, licensing, high tuition fees.
Ethical-economic discrepancy. On the one hand, medical care requires significant funds, and on the other hand, it is immoral to demand money for saving lives and restoring health. In economically developed countries, a historically developed mechanism is the availability of public medicine for the poor and insurance medicine for other segments of the population.
A feature of the market of medical services in countries with economies in transition is the exploitation by the private sector of fixed assets and human resources of the state segments, replenishing it. This process is effectively regulated in France. Physicians in public hospitals are allowed to work part-time in private practice at their hospital. Patients pay for medical services to the hospital administration, which deducts part of the doctors' fees for the use of equipment, premises and labor of nursing staff.
Consequently, some identified features of the health care market create restrictions for the operation of market mechanisms.
ITS PLACE IN THE GENERAL SYSTEM OF POPULATION NEEDS FEATURES OF CONSUMPTION OF GOODS AND HEALTH CARE SERVICES
The main purpose of the economy as an economy is to provide people livelihood and maintain the conditions of existence necessary for people. Main condition of existence a person is served by his health, therefore, maintaining the health of people is legitimately considered as one of the defining tasks of the economy.
The means of subsistence in conjunction with the conditions of existence are designed to satisfy the needs of people, including such a fundamental one as the need for health. Since the need for health cannot be satisfied directly, by producing and providing, selling to the consumer a product called "health", the economy is able to satisfy this specific need only through services and goods that promote the maintenance and promotion of health, prevent diseases and cure them.
Considering that the needs for health care services and goods are manifested and are in direct relationship with other needs of people, the state, society and form an integral part of this general system of needs, we will consider human needs as a whole, highlighting the group of needs we are interested in. At the same time, let us establish the place occupied by the needs for health care goods and services in the general system of personal, family, and social needs.
Everything that a person needs, that he needs, without which it is difficult or even impossible to live, is called needs. All people strive to satiate or, as economists say, to satisfy their needs. Things, objects, services with the help of which a person, family, people satisfy various, numerous needs, are usually called goods.
The need for health is undoubtedly one of the primary vital needs, the satisfaction of which is the main task of health care and is ensured by all its means, including economic ones. Therefore, health itself as a source of satisfaction of vital needs and medical methods and means of health care should be considered as benefits.
Some human needs, such as oxygen, water, partly heat, are met from natural sources. Nature itself has created the conditions of existence, thanks to which a person saturates such needs without much effort and expense, like animals. This freely available to allgood, for which you do not have to pay money or pay with labor, give other things in return. Man owes the presence of such free goods to nature. Concern for natural resources, protection of the natural environment, its restoration is a kind of payment for free benefits.
Natural sources in the form of fresh air, clean water, sunlight and heat also represent free goods that contribute to the preservation and promotion of health. This and much more is received by a person from nature in the form of natural medicines and methods of treatment. As accessibility decreases, such benefits are less and less free. In addition, due to the adverse environmental consequences of the production and economic activities of people, leading to environmental pollution, many types of natural benefits that people cannot do without become anti-benefits that undermine human health.
But many other needs, especially in food, clothing, shelter, movement, spiritual goods, can only be satisfied with the help of the means of subsistence created by people themselves. This, as mentioned earlier, economic benefits that people don't get for free. They
can only be obtained for money, through the expenditure of labor, or in exchange for other goods.
And can we consider economic, paid, say, medical services, schooling, free travel for pensioners and the disabled in public transport? And much more, for which all citizens or their individual categories do not pay money? Yes, these are economic benefits, for which not the one who receives them pays, but other people represented by the state, society. Such benefits are known as public.
Actually, one has to pay for free, natural benefits, spending efforts on picking up the fruits of nature, carrying out environmental protection measures. So there is no clear boundary between paid and free goods. The continuous increase in the needs of people, the increase in their diversity, on the one hand, and the limited possibilities for satisfying them due to the insufficiency of available sources, on the other, lead to an increase in the share of economic benefits in comparison with free, non-economic ones. Even natural water and clean air are becoming less and less accessible, more and more often you have to pay money for benefits that were free. More and more benefits a person receives not directly from natural sources, but through the economy, economic activity. The creation by people of the things they need, benefits is the main economic process, called production.
Created by people goods And services health care are, of course, economic benefits. Even medicinal herbs and medicines of natural origin, treatment through the use of thermal springs, mud, mineral water require preliminary efforts in the form of collection, preparation, arrangement, packaging, transportation and other procedures. Certain types of natural remedies used require the support of medical personnel. All this testifies to the economic nature of benefits in the form of goods and services used in health care.
The very processes of creating and using treatments are so closely related to the economy that it is appropriate to call them not the provision of services, but prodhealth leadership.
The use, application, use of goods, the saturation of needs, the satisfaction of needs in economic science are called consumption. The word "consumption" should therefore be understood in the broadest sense, meaning eating, wearing clothes, living in a house, driving a car, taking baths (consumption of services), and reading a book (consumption of spiritual goods). Consumption is the final process in the name of which the economy works, operates. It is legitimate to consider consumption as the goal of the economy, but with one significant caveat. It is necessary to consume exactly as much as is required for a full life, in volumes determined by the physiological needs of the body, the spiritual needs of the individual, rational, scientifically based standards. Otherwise, consumption can develop into unrestrained, harmful consumerism, those. consumption for the sake of consumption, and not for the sake of satisfying needs. Consumer trends often lead to the accumulation of goods in excess
quantity, beyond all measure, and besides, also unused. The causes of consumerism most often lie in greed, money-grubbing, immoderation
The consumption of health goods and services fits into the above general description of consumption, but at the same time has certain characteristics. If we are talking about medicines, special types of clothing and footwear for sick people, bandages, bandages, devices that facilitate the performance of vital functions, and other similar means, then consumption means in the economic sense use, useknowledge. Consumption of medical equipment means its usage in the process of diagnosis and treatment. The same applies to buildings, premises, equipment that form the fixed assets of healthcare organizations.
The situation is more complicated with the consumption of health services in the form of diverse activities of medical and auxiliary medical personnel. In health care they are called treatment, nursing. In the economy, the use of services, including medical ones, is commonly called service consumption, at the same time, this is understood as the receipt by the consumer of benefits in the form of the results of the activities of persons providing him with assistance, assistance, treatment, service.
In health care, the consumption of services is not always the final process in the full sense of the word. Services complete a certain type of production and treatment activity or stage of the treatment process. The rest, which completes the process, is the assimilation by the patient's body of the results of treatment. An indirect analogy is the consumption of food, which, strictly speaking, is completed by its assimilation by the body. The only difference is that the results of treatment are rarely absorbed as quickly and reliably as food. The consumption of certain types of health services, for example, diagnostic, consulting, health-improving services, can be legitimately considered the final procedure of the corresponding types of activity.
There is reason to talk about consumer trends in health care, watching the sick or even pseudo-sick, ready to spend the bulk of their lives in medical institutions without the need for it. In particular, overconsumption, harmful consumerism is manifested in the immoderate use or even abuse of medicines, unconditioned by the need for health.
Many people's needs are saturable in the sense that they can be sufficiently satisfied by known means. For example, it is quite enough for a person to consume a diet with a calorie content of approximately 2500 calories per day. Consumption beyond this limit of saturation becomes excessive, even harmful. Another thing is that people always want to consume more varied, tasty food. Or it is unlikely to have more than two refrigerators in the apartment. But the need for knowledge is limited by a clear boundary. The need for money is also included among the unsaturable, unlimited, although there is a known limit on the amount
money, quite sufficient for a comfortable existence of a person.
As for the needs for health care goods and services, they should, in our opinion, be classified as saturable. Even the original need
in health is satiated in the sense that the painless state of health of a person whose body normally performs its inherent functions may well be called the norm of health that sufficiently satisfies the needs for it. Accordingly, the saturation of the need for health care goods and services should be considered the possibility of obtaining them in quantity and composition, time and place, determined by the state of people's health and objectively necessary means of maintaining it. At the same time, the quality of methods and means of treatment, scientific knowledge about human health is not limited by a predetermined limit.
Are the needs of different people the same? It is obvious that certain needs, for example, for food, clothing, knowledge, are characteristic of all people, while others are far from being for everyone, but only for those who need them. The need for health is obviously inherent in all normal people, but the need for certain health services and goods is for those who need them. It seems that the need for modern diagnostics of the state of the human body, dangerous diseases, anti-epidemic measures, sanitation and hygiene, health-improving procedures are universal in nature, apply to all people (to a slightly different degree, depending on age, gender, health status, regional characteristics).
To a certain extent, the needs of a person, family, group of people, society differ. Therefore, allocate personal, family, group, communityneeds.
The needs for services and goods intended for the protection of human health, treatment, are mostly personal, individual in nature. The object of care, service, satisfaction of needs for medical supplies is ultimately a person, a person. The health of an individual is that elementary cell that makes up the level of health of families, social groups, the population of a region, a country. Therefore, the personal needs of a person in the means of maintaining health form the basis of the entire system of needs for health services and goods.
In addition, there are personal needs, due to the fact that in medicine a huge role is played by self-medication, home treatment under the supervision of doctors, and even self-treatment. Any person needs a home first aid kit in the form of a set of standard or individually designed medicines. Each person must have devices for measuring temperature, and in some cases - special equipment, the appearance of which is determined by the nature of the disease. The presence in every home of health-improving, sanitation and hygiene facilities has become a sign of medical and even general culture.
The category of personal needs in healthcare facilities should include the availability of elementary, common medical knowledge, household reference medical literature, the ability to recognize signs of a sudden widespread disease and provide the simplest emergency care. People who are prone to diseases or chronically ill need a means of calling for medical help.
In special cases, individual patients can afford to meet the need for a personal doctor, more often people use the services of family doctors.
Family medical needs may exceed the sum of the personal needs of each family member, since sometimes health and health problems arise that relate to the family as a whole due to, for example, hereditary diseases, the danger of spreading the disease of one of the family members to the whole family. Individual health care products, physiotherapy exercises, drugs may be the object of the needs of the whole family or several family members. This fully applies to the subjects of sanitation and hygiene.
For all the importance of personal and family needs for health care services and goods, such needs can be met almost in full, at the normative level, only when they become part of group, public needs. There are compelling reasons for such a conclusion.
Firstly, the provision of medical services individually to each person in need of them at home, through personal treatment, would require a significant increase in medical personnel, the delivery of treatment products to each individual, which would lead to a huge increase in costs and the cost of care.
Secondly, the provision of health care services in their public form makes it possible to concentrate medical staff, medical equipment, diagnostic and treatment tools, create favorable conditions for treatment and the provision of other services required by medical science within relatively narrow areas of polyclinics and hospital hospitals. This significantly improves the quality and reliability of service and treatment by making it complex, comprehensive and providing sterile conditions. In addition, with a collective, multi-personal service, cost savings and a better use of the production potential of clinics are achieved.
The reasons given are so significant that they give grounds for asserting the social nature of the bulk of the needs for health care. There is no doubt that the health of each person is of intrinsic value both for him personally and for the state and society. It is clear that the processes of treating patients are personally oriented, mass treatment is the exception rather than the rule. But the demand for health care services and goods is public character in the sense that they are characteristic of almost all people and can be fully satisfied only
3 using public forms. Thus, the consumption of health care products is predominantly mass public
And Rakter, has a social nature.
This thesis is also supported by the consideration that the same concerns
Evania, for all their specificity, is characteristic of many people, has
Etion to spread on a massive scale. Therefore, the treatment of one tre-
There is no cure for many in the same way that the treatment of many requires the treatment of Ka *Dogo of them.
The public need for health care arises as a result of the integration, connection and interaction of personal and family needs. With group, collective. The ship's crew needs a ship's doctor and a medical center, the population of the village - a small clinic, the city needs a variety of clinics, hospitals, doctors, and the country as a whole - a comprehensive health care system that can meet the needs of the entire population.
In economics, needs are usually divided into material and spiritual. material call the needs of people in things, objects, material values, while spiritual needs- this is the need for spiritual food in the form of knowledge, beliefs, cultural values, information, information about the world around us, intellectual communication.
Health needs are both material and spiritual in nature. Material and material needs include the need for medicines, clinical nutrition, medical clothing and footwear, material and technical means of treatment in the form of materials, energy, equipment, vehicles, devices, premises, buildings, structures. The need for the science of health, for medical knowledge, for information about diseases and methods of their treatment, for consultations, for a culture of health, for a healthy lifestyle should be considered spiritual.
These are fairly obvious truths. But it is not always so easy to classify health care needs as obviously material or spiritual. The problem is not solved in such a simple way with regard to the nature of health services in the form of essential medical activities in the process of treating patients. The need for an operation to remove or even replace organs and their parts is formally material in nature and is directly related to the application of physical effort. But it is inseparable from the spiritual need in the form of the initial establishment of the type of disease and the method of treatment. Examining the patient's examination data, listening to his complaints, prescribing a medicine, the doctor most likely satisfies the spiritual needs of the patients, but in the process of taking medicines, using other material means of treatment, the needs materialize, acquire a material form.
The thing is that health itself combines inextricably linked, interacting material and spiritual principles. Therefore, both the need for health and the need for healthcare facilities that provide it are of a complex material and spiritual nature. This connection is so strong that it is often not possible to separate the material and spiritual aspects of health services. This is one of the most characteristic features of health care services, the needs for them and the processes of their consumption, which distinguishes the health care economy from the category of very specific sectors of the economy and the service sector.
Usually, it is customary to rank people's needs, establishing a measure of importance, significance of a particular group of needs in the general hierarchy, often depicted as a "needs pyramid". Sociologists quite often place at the top of such a "pyramid" the need of people for self-realization, self-expression, self-affirmation, and at the base of the pyramid -
physiological needs, considered as the simplest, are not so
chimy and important. At the same time, the need for health and healthcare is not
ZN is separated as independent, but is included in the need for security
The nursery should proceed from the fact that the need for health and its protection is
essential character and without its satisfaction other needs cannot
be realized, then this need deserves the highest place.
Since health is initially present in a healthy organism, psycho-
until the need for health becomes adequate to the need for life
Only by virtue of the loss of health comes the realization that the physical and
spiritual health is the main, main life value.
Questions
What are needs and how are they related to the conditions and means of existence
people?
Name the main types of benefits and sources of their receipt.
How are the production and consumption of goods in the form of goods related?
and services?
Describe the types of needs of a person, family, society in interconnection
with health economics.
What is the social nature of health care needs?
How are material and spiritual needs related?
What does the “pyramid of needs” mean and how is it built?
Consumption, satisfaction of needs, representing the ultimate goal of the economy, are inextricably linked with production, that is, with the creation of an economic product that is then consumed. Production not only ensures current consumption, but also creates the opportunity to recreate and reproduce the consumed product of production activity again and again. The processes of treatment, health care are usually not called production, although in reality health care is nothing more than the production of medical services or (in a broader sense, the production and reproduction of people's health).
The production processes in the economy are as continuous as the life of the people of society, which they are called upon to provide with the necessary means of subsistence. The economy, the core of which is production, is dynamic. The development of the economy, the change in its conditions are due to a number of reasons.
Firstly, the natural source of Economics - nature - is changing, constantly exhausted. So you have to limit consumption
natural resources, create interchangeable, restore renewable resources.
Secondly, it is necessary to constantly maintain the consumption of people's means of subsistence and the conditions of their existence. So the "production boiler" must cook more and more new food. Moreover, due to the growth in the number of people - consumers and the increase in their needs, it is necessary to prepare more and more voluminous and tasty "economic food". And just as the existence of people, society, does not stop for a minute, cannot interrupt its operation and the production economy - the life support system.
Thirdly, all man-made, the economy in the form of a "second nature" - the means of production and infrastructure - is constantly wearing out. A dynamic economy is designed to recreate and reproduce the anthropogenic nature.
Fourth, scientific, technological and social progress stimulates people to look for new ways and means of production, improve their lifestyle - this is another incentive for the economy to continuously function.
The economy, therefore, is called upon not to be at rest, but to act, to work for the people and in the name of the people. Economic actions also include the production activities of the people themselves, their interaction with the means of production and among themselves. Production leads to the transformation of economic resources into the economic product needed by a person, society.
Factors of production
The economic resources involved in the production process begin to play the most active role in it, turning from a source into a participant in production. To emphasize this important circumstance, it is advisable, along with the concept of "production resources", to use the concept of "factors of production". Under production factors understand the types of economic resources that are used in production, become participants in it, affect the quantity and quality of the product produced, including the production of health services.
In economic theory, quite often the concepts of "production resources" and "factors of production" do not differ, they are considered identical. This view implies that the factors of production are formed from economic resources. And yet there are certain differences between the factors of production and production resources. A resource is something that can be used, something that is intended for use, and factors - something that affects production, is used in production processes, including in production activities, the provision of services.
In economics, the three factors of production that have become classic are widely known: land, labor, capital.
Land as a factor of production is not only land in the proper sense
ova, that is, land and the location of production facilities - the Earth is understood in a broad sense as the totality of all natural
cvpcoB planet Earth involved in the production process. These are arable land, other agricultural land, land under the object-industrial purpose, minerals, water resources, air pool, vegetable and animal world nature. Since health care uses natural resources, and natural conditions affect health, the natural factor plays a significant role in the health economy.
Labor, understood as a factor of production, is the employed labor force, that is, the part of the population participating in production activities. Labor - a production factor - is usually measured by the number of workers employed in production, or the amount of labor time spent by these workers. At the same time, the quality of labor, its productivity, and returns are also taken into account. In health economics labor factor plays a decisive role. The volume and quality of medical services provided, the degree of satisfaction of needs for them, and the effectiveness of treatment directly depend on the quantitative and qualitative composition of medical personnel.
Capital is the third factor of production. It is understood as the means of production created by people, used to obtain the manufactured product. This is, first of all, fixed assets in the form of industrial buildings, structures, equipment, instruments, apparatus. It is customary to include production as capital. infrastructure in the form of means of communication, communication, heat, energy and water supply.
In economics, the main means of production, considered as a factor of production, are called physical capital, to emphasize its material, material nature. In practical, applied economics, fixed assets are also called main funds.
In the health economy, capital goods play an important role because:
the presence of buildings and structures, equipment determines the number of places (pain
beds) in hospitals, and in polyclinics - throughput, -
all this affects the comfort of treatment;
the availability of instruments, equipment determines the quality and efficiency
treatment;
The word "capital" is also tied to money, understood as
lower capital. However, money capital, unlike physical capital, does not
It is customary to consider it a factor of production, since money itself is in pro-
do not participate in leadership. But money capital, called investment
And or investments, used to purchase fixed assets
ic capital, becomes a tangible, important factor of production
> especially when it comes to expanding it, increasing the
A > competitiveness.
Considering the concept of "production capital" in a broad sense, it should be added to fixed capital negotiable in the form of current, rapidly expendable resources of production. The need for working capital is often acute in medical organizations, and in terms of its importance, this capital should be included in the third factor.
In addition to these three leading factors of production, one more, fourth factor is often mentioned in modern economic literature. This entrepreneurship, entrepreneurial activity, entrepreneurship. Entrepreneurship characterizes people who are actively involved in production and in production management, who are able to effectively, optimally use economic resources in order to obtain the highest results. Entrepreneurial ability organizers and participants in production allow, with the same economic resources, to obtain an economic product in a larger quantity and best quality. If the volume of production is given, then, thanks to the entrepreneurial factor, it is possible to reduce the amount of resources expended, to carry out production at lower costs, using resource-saving technologies and progressive methods of organizing labor and production.
In the process of establishing market relations in the Russian economy and partly in health care, an idea arose of entrepreneurship as a private sector that diverts funds, factors of production from the state, public sector. Meanwhile, the essence of entrepreneurship is different. It is designed to inspire initiative, direct efforts to find ways to more fully, better, more affordable meet the needs for medical goods and services in comparison with the level provided by public medicine.
can also be considered as a factor of production. scientific and technical potencial, characterized by the degree of education, professionalism of workers, the progressiveness of the means of production used, the use of scientific achievements in production. The scientific and technical and technical and technological potential of health care is one of the main criteria for the ability of the health care system to fulfill its main purpose.
Knowledge of the factors of production makes it possible to assess the production capabilities of the economy as a whole and its individual links, such as the health care economy.
Action production system
Since the economy is designed to produce what people need, its main function is to production final and related intermediate economic product. Economic objects involved in production, and the production processes taking place in it are called productionNoah system. The simplest structure of the production system and the scheme of its operation are shown in fig. 3.
This is a general, enlarged scheme of production related to any type of production and economic activity. The specifics of the production

Rice. 3. Scheme of the production system.
of the health care system lies in the way in which productive resources are transformed into an economic product of productive activity, and in the nature of the product itself. Such a transformation always occurs in the process of production activity.
From Everyday life household appliances are well known for converting one type of product into another. Having turned meat, bread and onions in a meat grinder, we get minced meat. Putting meat, potatoes, cereals and salt in a pot of water, pouring water over them and boiling them, the cook will cook meat soup as a result. By putting firewood into the stove and burning it, we get heat.
The manufacturing economy operates in a similar way. Economic resources are fed into it, and as a result of the production transformation of which an economic product is created. Of course, the analogy between a production system and a meat grinder or a saucepan is largely arbitrary. In production, we are not dealing with the transformation of one type of resource, let's say material, into one type of product, but a wide variety of resources into a variety of products, and in a variety of ways.
Economic resources include both natural and labor, and means of production (tools and objects of labor), and information. All these resources enter the production system and mix and combine in it. But this is not a mechanical connection, but the production interaction of resources of different origin. Labor resources, using fixed assets and information, applying a variety of technologies for processing natural resources, raw materials, materials, energy, ensure the creation of the necessary product of the required quality. So the production process as a whole is much more pure and diverse than a specific type of transformation of one material into another. And yet the general scheme of operation of the production system is reminiscent of the process of turning one thing into another. in Healthcare, the work of medical workers in its unity and interaction with equipment, preparations, sources of matter and energy, acts on the human body, ensures the maintenance, strengthening, restoration of health through the production of diagnostic results, medicine Nnghh means, updated organs, living conditions, and in the long run - health itself. Of course, Dicine's production activities are very specific in that the transformation of resources
covers the involvement of a person - the object of treatment, in the process of transformation. In addition, the produced product is also exceptionally original, which can be informational (diagnosis), material (drug), physiological (physiological changes in the body achieved through treatment), a new or renewed organ (the result of an organ transplant, surgery, drug exposure), improvement in health status.
At the beginning of the working day, many millions of people go to enterprises, institutions, their jobs, ready to realize their labor abilities. As soon as these people begin to perform their work duties, they become workers, production participants, part of the production transformation that turns resources into an economic product. Those involved in the production process workforce, representing the most important, creative part of the resources of production. In healthcare, the workforce is represented by medical staff, scientists, support staff, employees of the administrative apparatus.
In the course of their work, employees use fixed assets of production(sometimes called fixed assets) in the form of buildings, structures, machines, equipment, tools. As soon as the worker turns on the device, unit, machine, these resources become integral part production transformation. They contribute to production and themselves participate in the transformation of production resources into a manufactured product, gradually wearing out, partially devoting themselves to the goals of production. Fixed assets represent material and material resources of production, along with others material resources, such as the materials used in production and the energy that forms working capital. IN unlike fixed assets, current assets are fully used during one production cycle (for example, dressings, a syringe, a portion of a medicinal product), that is, they are not used repeatedly.
The production process captures, "sucks" Natural resources in the form of natural resources. People are involved in the production of many types of minerals, flora and fauna of nature, water, air, earth. Thus, natural resources are converted into working capital: raw materials, materials, fuel, energy, which enter the converter and become participants, components of production. They are the material basis of the economic product.
Medical production activities directly use natural resources such as medicinal herbs, mineral water, healing springs, mud, natural means of recreation. At the same time, natural resources material basis creation of tangible means used in medicine.
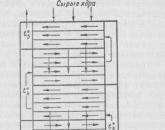



Popular
- Where to get start-up capital for a business
- How to name a company: examples of names
- Making money in Sims
- How to make money while traveling How to make money while traveling
- All profitable business niches
- All profitable business niches
- Top bucks that pay in dollars
- Earning on comments
- Similar to vktarget. Vktarget reviews. How to get more tasks on the VKtarget project - basic recommendations
- How to start earning in the game Farm Neighbors?